Microbes that live and actively grow in a specific area are called the resident microbiota (or resident flora). These are the microorganisms that have stably colonized a particular site, whether that's a patch of human skin, a stretch of your large intestine, or a layer of soil, because the conditions there consistently support their survival and reproduction. They are not passing through. They are not accidental contaminants. They belong there, in the biological sense, because that environment gives them exactly what they need: the right temperature, pH, moisture, oxygen level, and nutrients to keep growing and holding their ground.
Microbes That Live and Grow in an Area: Normal Microbiota
Marcus Holloway
21 Jun 2026

What 'microbes that live and grow in a certain area' actually means in microbiology

When a microbiology textbook or a clinical reference says a microorganism 'lives and grows in a certain area,' it is describing stable, long-term colonization of a specific ecological niche. That niche might be a body site, a section of soil, a water surface, or the interior of a biofilm. The key idea is persistence: the microbe is not just detected there once, it is reliably present over time because the local conditions consistently favor its growth.
This is worth separating from two things it is often confused with. First, it does not automatically mean the microbe is causing disease. Most microbes living stably in and on the human body are harmless under normal circumstances, and many are actively beneficial. Second, it is different from temporary presence, where a microbe lands somewhere, survives briefly, and then disappears without establishing itself. That second category has its own name, which we will get to shortly.
The correct microbiology terms: normal microbiota, resident flora, and what 'endemic' does not mean here
The most precise term for microbes that live and grow stably in a particular area is resident microbiota (sometimes written as resident flora, especially in older clinical literature). The Merck Manual defines resident flora as the microorganisms that usually occupy a particular body site. The broader term 'normal microbiota' refers to the entire community of microorganisms that colonize a healthy individual, covering all body sites together. You will also encounter 'normal flora,' which means the same thing and is still widely used, though it is slowly being replaced by 'normal microbiota' in current scientific literature.
There is also a terminological split worth knowing. 'Microbiota' refers to the actual microbial taxa associated with a host or environment. 'Microbiome' technically refers to the full catalog of those microbes and their collective genes, though in everyday scientific conversation the two words are often used interchangeably. The American Society for Microbiology describes the microbiome as a community of microorganisms living on, in, and around people and other environments, including soil, oceans, and the atmosphere. So when someone says 'the gut microbiome,' they mean both the community of resident microbes and the genetic information encoded in that community.
One word that causes real confusion is 'endemic.' In disease epidemiology, endemic means a disease or pathogen is consistently present at a baseline level in a population or geographic region. That is a different use of the word. In the context of microbes living in a niche, microbiologists do not typically use 'endemic' to describe normal residents. Stick with 'resident microbiota' or 'normal flora' to avoid that mix-up.
The direct contrast to resident microbiota is transient flora, defined as microorganisms that colonize a person (or a surface) for hours to weeks but do not establish themselves permanently. Transient microbes are present by circumstance, not by ecological fitness for that site. Understanding this resident-versus-transient distinction is genuinely useful, not just for exams, but for making sense of hygiene, food safety, and clinical risk.
Where 'a certain area' can be: body sites and environmental niches

The 'area' in this context can be almost any defined space with consistent physical and chemical conditions. In human microbiology, the classic examples are specific body sites, each of which hosts a distinct resident community.
- Skin: Staphylococcus epidermidis is a dominant resident, sometimes making up more than 90% of the aerobic resident flora in certain skin zones. Cutibacterium acnes (previously classified as Propionibacterium acnes) thrives in sebaceous, relatively anaerobic follicular environments.
- Gastrointestinal tract: The colon is the most densely colonized site in the human body, dominated by anaerobic bacteria that ferment dietary fiber into short-chain fatty acids like acetate, propionate, and butyrate.
- Stomach: Bacterial loads are kept very low (roughly 10^3 to 10^6 organisms per gram) by the acidic environment, so most organisms passing through the stomach are transient rather than resident.
- Oropharynx: A rich and complex resident community, including streptococcal species and many anaerobes, established early in life.
- Vagina: In healthy adults, Lactobacillus species typically dominate, producing lactic acid that keeps pH low and discourages colonization by other organisms.
- Eyes and nasal passages: Also host distinct resident communities shaped by local moisture, antimicrobial secretions, and mechanical clearance mechanisms.
Environmental niches work on the same principle. Soil microbiota are shaped by mineral composition, organic matter content, moisture, and oxygen availability. Aquatic biofilms on rocks or pipes develop resident communities anchored to surfaces. Deep-sea hydrothermal vents host thermophilic and chemolithotrophic residents that would die at ordinary surface conditions. In every case, the resident microbes are those whose growth requirements match what that specific area consistently provides.
What actually lets microbes persist in a specific area
No microbe settles into an area by accident. Persistence requires a match between the microbe's growth requirements and the area's physical and chemical conditions. For example, bacteria that can grow on minimal medium are often described as minimal-medium bacteria, which helps characterize what kinds of nutrients they require bacteria that can grow on minimal medium are called. The main factors are temperature, pH, and moisture (water activity). Think of these as the baseline admission criteria for any niche.
Temperature
Most microbes that colonize warm-blooded animals are mesophiles, meaning they grow best roughly between 20°C and 45°C (68°F to 113°F), with an optimum near 37°C for human-associated species. For example, microbes that grow best at around 37°C are classified as mesophiles, which fits many human-associated species. That is exactly why body-site residents are almost all mesophiles: the human body maintains a temperature right in their sweet spot. Psychrophiles (optimum near 0 to 15°C) and thermophiles (optimum above 50°C) do not colonize human tissue for the same reason a tropical fish does not thrive in a mountain stream. Environmental niches, like refrigerated food surfaces or composting piles, select for the temperature category that matches their conditions.
pH
pH is one of the most powerful sorting mechanisms in microbiology. The stomach's acidity (pH roughly 1.5 to 3.5) keeps bacterial loads extremely low, which is why the stomach has few true residents compared to the near-neutral colon. The vagina's low pH, maintained by Lactobacillus-produced lactic acid, is what makes Lactobacillus dominance self-reinforcing: the residents create the acidic conditions that favor their own continued growth while discouraging competitors. Skin sits at around pH 4.5 to 5.5, which favors acid-tolerant residents and offers some resistance to less-adapted transient organisms.
Moisture and water activity
Water activity (written as aw) measures how much of the water in an environment is actually available for microbial use, on a scale from 0 to 1. Most fresh foods have aw above 0.95, which means bacteria, yeasts, and molds can all grow freely. The FDA considers foods above approximately 0.86 aw to be potentially hazardous from a microbial growth standpoint. Below 0.6 aw, even osmophilic yeasts cannot grow. On the body, moist skin folds (axillae, between toes) support denser microbial communities than dry forearm skin, for exactly this reason. Dehydrating food or drying surfaces is one of the most reliable ways to eliminate resident microbial growth, because you are removing the water activity that colonizers depend on.
Oxygen and growth mode: aerobic, anaerobic, and the microenvironments in between

Oxygen availability is another major filter that determines which microbes can establish themselves in a given area. The key categories are worth knowing clearly, because they explain a lot about why certain organisms live where they do.
| Growth type | Oxygen preference | Where they tend to reside |
|---|---|---|
| Strict aerobes | Require oxygen | Skin surface, upper respiratory tract, open wounds |
| Facultative anaerobes | Grow with or without oxygen | Gut, skin, many food surfaces |
| Strict (obligate) anaerobes | Killed by oxygen | Deep colon, dental crevices, deep wound tissue |
| Microaerophiles | Prefer low oxygen (roughly 1–10%) | Gastric mucosa (e.g., Helicobacter pylori), certain gut niches |
| Aerotolerant anaerobes | Can survive oxygen but do not use it | Intestinal tract alongside strict anaerobes |
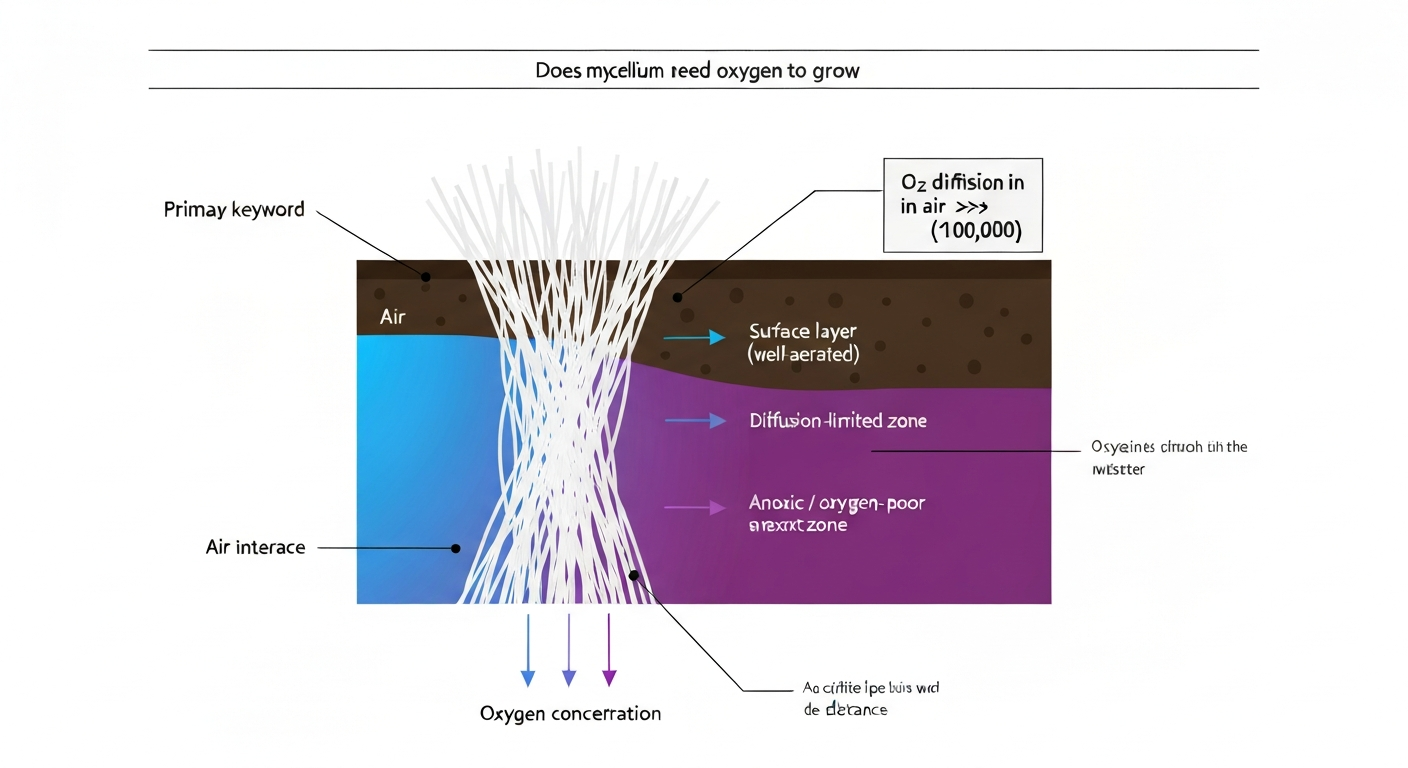
The colon is one of the best examples of oxygen-driven niche separation. The lumen of the large intestine is essentially anoxic, which is why strict anaerobes dominate there and make up the vast majority of the gut microbiota. Move to the gut mucosal surface and you find a slightly higher oxygen gradient, which supports a different, more oxygen-tolerant community. This layering is not random; it is determined by the oxygen microenvironment at each precise location.
Biofilms illustrate this beautifully at a smaller scale. In a biofilm (a structured community of microbes attached to a surface), oxygen is consumed at the outer layers, creating steep oxygen gradients inward. Educational resources from the Center for Biofilm Engineering also describe how oxygen-depleted or anoxic regions can occur within biofilm structure, such as in microcolonies, because gradients develop inside the biofilm oxygen-depleted or anoxic regions within biofilm structure. The result is that strict anaerobes can live comfortably in the interior of a biofilm even on an exposed surface, because the outer aerobic community has already depleted the oxygen before it penetrates deeper. This is why biofilms in pipes, on medical devices, and on teeth harbor complex, mixed-oxygen communities.
Nutrients, competition, and why some microbes stay while others cannot
Even if temperature, pH, moisture, and oxygen are all favorable, a microbe still has to compete for nutrients and physical space to become a true resident. Can prototrophs grow on minimal media depends on whether they have the biosynthetic pathways needed to make all required compounds from basic nutrients growth requirements. This is the ecological side of colonization, and it is why the 'area' matters just as much as the microbe's individual growth requirements.
The gut microbiota is a great model here. Resident gut bacteria ferment dietary fiber, producing short-chain fatty acids that feed colonocytes and shape the gut environment. They also produce bacteriocins (antimicrobial proteins), fatty acids, and other inhibitory metabolites that actively suppress would-be colonizers. The Merck Manual and multiple microbiome reviews describe this as colonization resistance: the resident community uses up available nutrients, occupies binding sites, lowers pH, and secretes inhibitory compounds to collectively resist invasion by outsiders, including pathogens like Clostridioides difficile. Secondary bile acids produced by resident gut bacteria, for example, actually inhibit C. difficile spore germination. When the resident community is disrupted (often by antibiotics), that resistance drops and opportunistic pathogens can move in.
Skin residents operate by the same principle. Staphylococcus epidermidis, the dominant aerobic skin resident, does not just passively occupy space. It produces bacteriocins and antimicrobial peptides that can reduce colonization by Staphylococcus aureus, a much more dangerous organism. The commensal is actively defending its niche, and in doing so it protects the host. This is why randomly killing off all skin bacteria with harsh antiseptics can sometimes make things worse, not better: you remove the protective competition.
Nutrient availability also explains why different body sites host different communities. The skin surface is relatively nutrient-poor, favoring slow-growing, lipid-metabolizing organisms like Cutibacterium. The colon is nutrient-rich (especially in fermentable carbohydrates), supporting an enormous and diverse anaerobic community. The stomach, with its harsh acidity and rapid transit, barely supports any permanent residents at all. Matching nutrient availability to microbial metabolic strategy is central to understanding why each area has its own characteristic microbiota.
Practical takeaways for hygiene, food safety, and controlling microbial growth
Understanding resident versus transient microbes is not just academic. It has direct, practical implications for how you handle hygiene and food safety decisions.
For food safety, the key insight is that bacteria grow most rapidly between 40°F and 140°F (roughly 4°C to 60°C), which the USDA calls the 'danger zone.' Food left in this range for more than two hours (or one hour if ambient temperature is above 90°F) accumulates enough microbial growth to become a risk. Lowering temperature (refrigeration at 40°F or below), reducing water activity (drying, salting, sugar preservation), and adjusting pH (acidification, fermentation) are all ways to remove the conditions that let microbes persist and grow. They work because they take a niche that was hospitable and make it hostile.
For hygiene, the resident-versus-transient distinction shapes strategy. Routine handwashing targets transient flora: the microbes picked up from surfaces, other people, or contaminated objects. These are relatively easy to remove with soap and water or alcohol-based hand sanitizer because they are not firmly attached. Resident hand flora (organisms that colonize skin deeply and persistently) are much harder to eliminate with normal washing.
The CDC notes that surgical hand preparation is specifically designed to reduce resident flora before procedures because those residents, not just transient contaminants, become a risk when sterile tissue is exposed. Approximately one million skin cells carrying viable microorganisms are shed from the body every day, which gives you a sense of the ongoing microbial traffic between skin and environment.
It is also worth noting that being a resident does not mean being harmless in all circumstances. Normal flora from skin, the oropharynx, the GI tract, or the genitalia can cause serious infection if they reach normally sterile sites, such as the bloodstream, joint spaces, or the peritoneum, especially in people with impaired immune defenses. A microbe that is a well-behaved resident in its normal niche can become a pathogen when it crosses into an area where it does not belong.
How to tell normal residents from temporary contaminants, and when it matters
In practice, distinguishing a resident from a transient is about asking whether the microbe's presence makes ecological sense for that site. A few guiding questions help.
- Is this organism consistently found at this site in healthy individuals? If yes, it is likely a resident. S. epidermidis on skin or Lactobacillus in the vagina are expected findings, not contamination.
- Does the organism match the growth conditions of the site? Finding an obligate anaerobe on a dry, well-oxygenated skin surface is a flag that something unusual is happening. Finding it in a deep wound or the colon makes complete sense.
- Is the organism present in high numbers or low numbers? Residents are typically present in stable, relatively high numbers. Transients are often present in low, variable numbers and disappear on repeat sampling.
- Is the organism present across multiple samples over time? Residents persist. Transients come and go.
- Is the organism causing signs of infection, or is it simply present? Colonization (stable residence without disease) is fundamentally different from infection (tissue invasion with host damage), even though the same organism may be responsible for both in different contexts.
In clinical microbiology labs, the resident-versus-transient question comes up constantly when interpreting culture results. A positive blood culture for S. epidermidis, for example, requires careful interpretation: is this a genuine bloodstream infection, or is it a skin contaminant introduced during blood draw? The answer depends on whether multiple cultures are positive, whether the patient has risk factors (like an indwelling catheter), and whether the clinical picture fits. That is exactly the resident-versus-transient distinction applied in a high-stakes setting.
For students and educators, the most useful way to anchor this concept is to always tie the 'area' back to its conditions. Ask: what is the temperature there, what is the pH, how much oxygen is available, how much moisture is present, and what nutrients are on offer? Knowing the temperature there also helps explain why many bacteria grow best around 37 degrees Celsius, which is close to human body temperature. Those five factors together predict which microbes can establish themselves as residents and which ones, however frequently they land there, will never truly take up residence. That predictive framework is what makes microbiology practical rather than just a list of names to memorize.
FAQ
If microbes live and grow in an area, does that mean they never change?
A microbe can be “resident” and still change over time, like after antibiotics, illness, diet shifts, pregnancy, or aging. In those cases, the site conditions remain similar, but the community composition moves toward a different stable equilibrium.
Can a resident microbe still cause disease?
Yes. Even when a microbe is a normal resident, it may be harmless on the skin but dangerous if it enters a sterile site. For example, organisms common on skin or the GI tract can cause serious infection after surgery, trauma, or catheter-related spread.
How do you know it is truly “resident” and not just detected there?
No. Detecting DNA or RNA from a sample does not guarantee active growth or stable colonization. A resident microbiota should be consistently present and ecologically supported by the site conditions, while “present” alone could reflect recent deposition.
Does “resident” mean the microbe is always beneficial?
Resident and transient microbes are not the same as “always good” versus “always bad.” Some residents suppress pathogens and some residents can become harmful under specific circumstances, such as immune suppression or breaches in barriers.
Why do some body areas have many residents while others have few?
It depends on the site. The stomach is strongly filtered by acidity and rapid transit, so it has fewer true long-term residents. Other sites like the colon have more stable communities because nutrients and oxygen gradients support persistence.
Why can a transient microbe survive for a while but still not become established?
Not necessarily. Transient microbes often survive for a limited period because they tolerate the conditions, but they cannot persist due to lack of competitive advantage, nutrients, attachment niches, or failure to establish at the right micro-oxygen level or pH.
How does oxygen availability determine which microbes become residents?
Oxygen is especially important in niches with strong gradients, like the gut mucosa versus lumen, and in biofilms where the inner layers become low-oxygen. A microbe’s “oxygen strategy” can determine whether it can persist at that exact depth or surface region.
If I dry or refrigerate a surface, do I eliminate resident microbes?
If you increase drying, salting, or refrigeration, you can reduce microbial growth conditions, but you may not remove all residents instantly. You are usually shifting the niche so residents decline or enter a less active state rather than instantly erasing them.
Why doesn’t handwashing completely sterilize skin?
Soap and water mainly remove and dilute transient microbes, but they do not reliably sterilize deeper skin layers or established biofilm-like habitats. That is why skin recolonization happens quickly after washing, even when transient risk drops.
Why do antibiotics sometimes lead to overgrowth by opportunistic pathogens?
Colonization resistance is strongest when the resident community is intact. Antibiotics can reduce diversity or eliminate key functional groups, which lowers inhibition and nutrient competition, allowing opportunists to expand even if the niche conditions still seem similar.
In lab results, what’s the practical way to avoid mistaking contamination for a real resident infection?
A single culture result can mislead because sampling technique and timing matter. Multiple specimens, repeated positives, and matching the organism to the likely exposure route and patient context help distinguish contamination or transient presence from true resident-associated infection.
Is an “endemic” microbe the same thing as a resident microbiota?
The word “endemic” refers to how often a disease or pathogen occurs in a population or region, not to whether a microbe is stably occupying a niche. A pathogen can be endemic in a community without being a resident microbe of every individual’s body site.